I am often emailed by yoga teachers and students who have been diagnosed with an “anteriorly tilted pelvis”, frequently being told that this is the cause of their persistent back pain. They usually want to know how yoga can help correct it.
The basic anatomy of the pelvis
Before we talk about tilt, correction, or pain, it helps to revisit the basic anatomy of the pelvis and what it is designed to do.
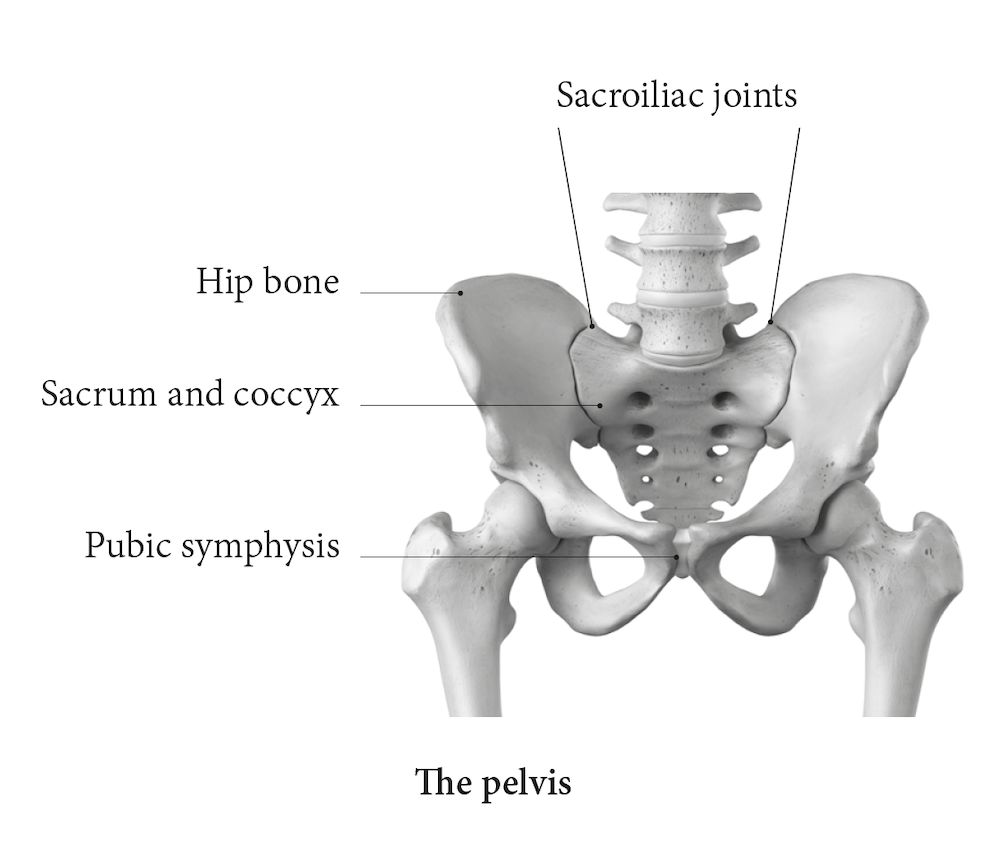
The pelvis is formed by the two hip bones, the sacrum, and the coccyx, creating a bowl-shaped structure, the word pelvis comes from the Latin for basin. These bones are strongly united, forming a largely immobile, weight-bearing structure. The pelvis connects the lower limbs to the axial skeleton via the sacroiliac joints and therefore plays an important role in movement and load transfer.
The bony pelvis also provides attachment and support for pelvic muscles and connective tissues, which in turn support the pelvic organs.
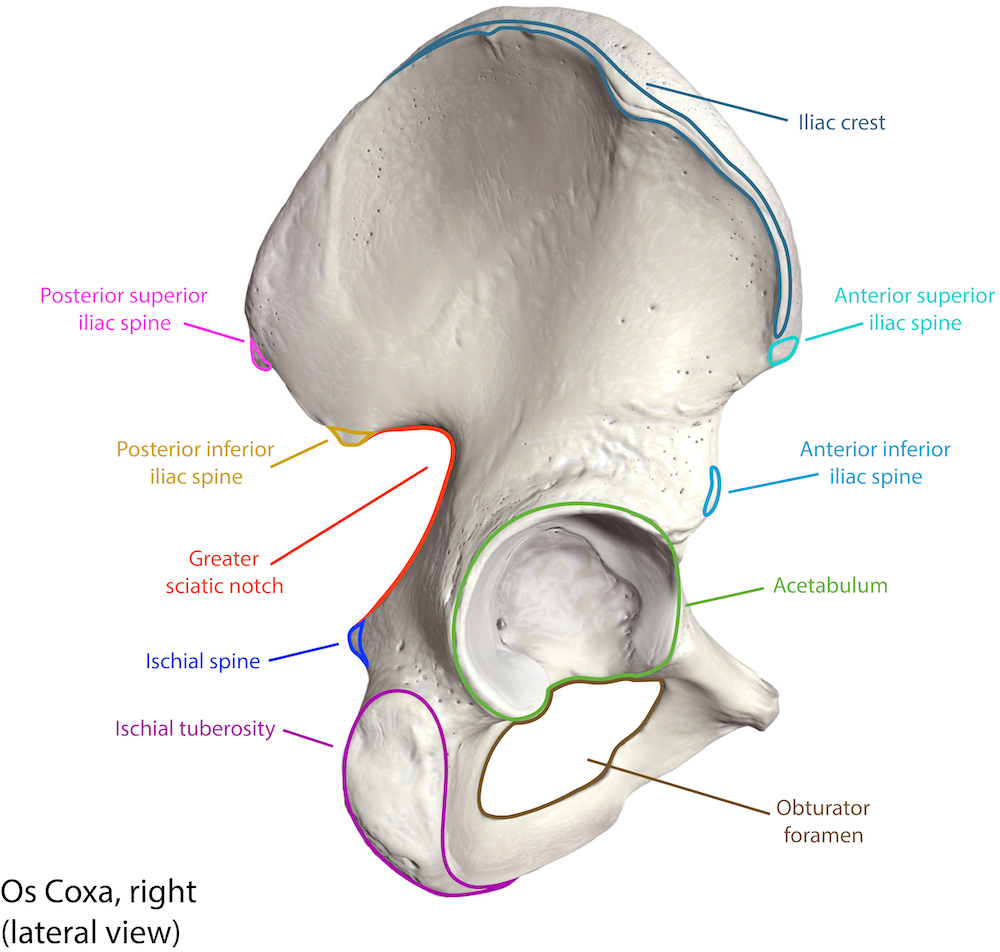
In the immature skeleton, each hip bone consists of three separate bones, the ilium, ischium, and pubis. Fusion typically begins between the ages of 14 and 16 and is usually complete by around 23 years of age (Moore, 1992). The acetabulum, the cup-shaped hip socket, forms at the junction of these three bones.
The superior curved margin of the ilium is the iliac crest. You can palpate it by placing your hands on your waist and pressing down slightly. The anterior end of the iliac crest forms the anterior superior iliac spine, or ASIS, which can be felt on the front and side of the pelvis. Just below it lies the anterior inferior iliac spine, or AIIS. Both serve as attachment sites for muscles of the thigh.
Posteriorly, the iliac crest curves downward to the posterior superior iliac spine, or PSIS. This landmark is not covered by muscle and is often visible as a small dimple in the lower back. Inferior to it lies the posterior inferior iliac spine, or PIIS. The PSIS and PIIS provide attachment points for strong ligaments and muscles supporting the sacroiliac joint.
The most prominent landmarks on the ischium are the ischial tuberosities. These are the attachment sites for the posterior thigh muscles and bear body weight in sitting. They are commonly referred to as the sitting bones, or sitz bones, from the German verb sitzen, meaning to sit.
What does pelvic tilt actually mean?
When teaching pelvic tilt, I find the image of a bowl of water helpful. If the bowl tips forward and water spills out the front, this represents anterior pelvic tilt. If the bowl tips backwards and water spills behind, this represents posterior pelvic tilt.
However, no two pelvises are the same shape or size, and no pelvis is perfectly symmetrical in any plane. A quick glance at anatomical images makes this obvious. What looks or feels neutral for one person may look and feel very different for another.
Pelvic tilt is often quantified by measuring the angle between the horizontal and a line connecting the ASIS and PSIS. Even this measurement varies widely across individuals. This raises an important question for teachers, how meaningful is it to label a pelvis as anteriorly tilted when every pelvis is unique?
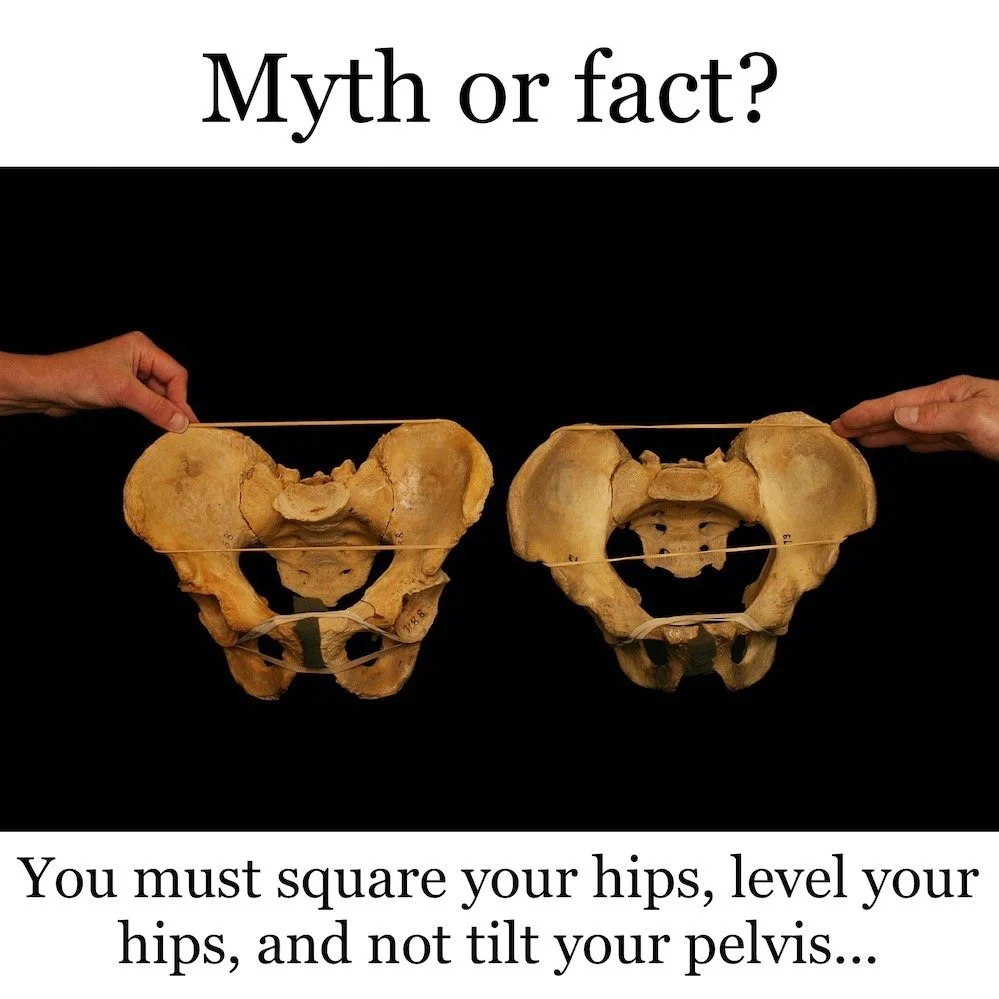
Image credit: Paul Grilley, paulgrilley.com
Is anterior pelvic tilt the cause of back pain?
This is where the story often becomes oversimplified. If posture alone caused pain, the picture would be much clearer than it is.
Herrington (2011) studied 120 adults with no lower back or pelvic symptoms. He found that 85 percent of males and 75 percent of females presented with an anterior pelvic tilt. Only a small percentage were classified as posteriorly tilted, and a minority were described as neutral.
In other words, anterior pelvic tilt was extremely common in people without pain.
For yoga teachers, this is an important reminder. Postural labels are poor predictors of pain. Seeing or feeling an anterior pelvic tilt does not automatically mean something is wrong, nor does it tell us what someone should change.
A more useful teaching lens
Rather than fixating on the shape of an asana or on achieving a particular standing posture, it can be far more valuable to help students explore movement options. Subtle and gross pelvic movements, changes in load, breath, and context often tell us more than static alignment cues.
There is a quote, often shared in yoga spaces, whose original source I have not been able to trace:
“Use yoga asanas to get into the body and not the body to get into yoga asanas.”
For teaching, this mindset shifts the focus from correcting shapes to cultivating awareness, adaptability, and confidence.
The next time you practise or teach, invite exploration. Experiment with pelvic position and notice how it affects sensation, effort, balance, and breathing in different asanas. This approach respects anatomical variability and supports more inclusive teaching.
References:
Herrington, L. (2011). Assessment of the degree of pelvic tilt within a normal asymptomatic population. Manual Therapy, 16(6), 646–648.
Moore, K. L. (1992). Clinically Oriented Anatomy (3rd ed.). Baltimore: Williams and Wilkins.