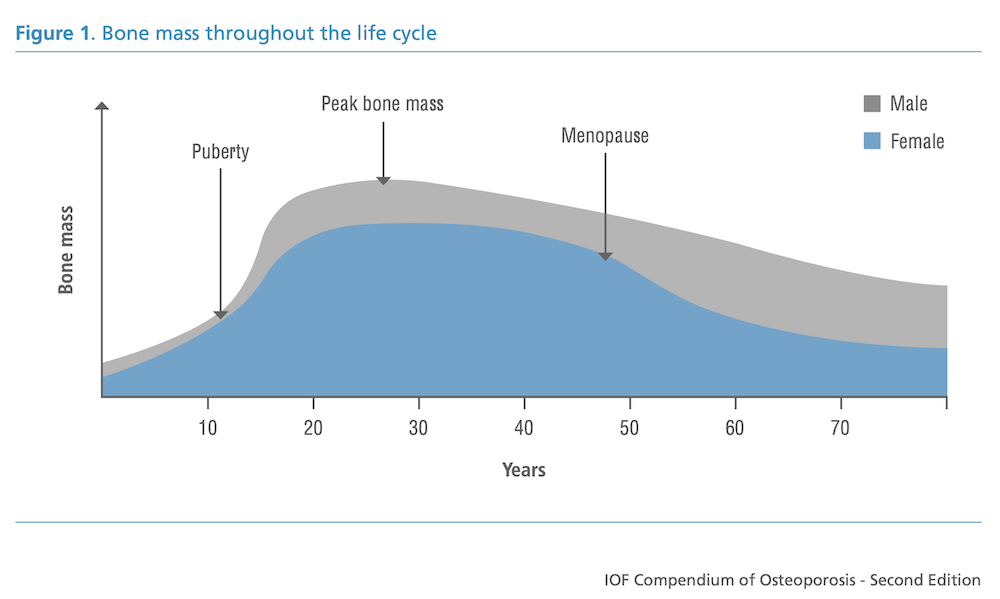
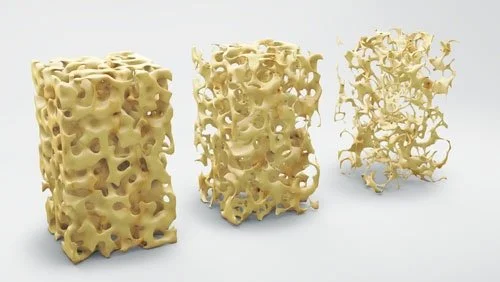
Over a person’s lifespan, bone is acquired during growth, reaches peak bone mineral density in early adulthood, and is gradually lost with advancing age (US Department of Health and Human Services, 2004). Osteoporosis is a systemic skeletal condition characterised by low bone mass and deterioration of bone microarchitecture, which increases bone fragility and fracture risk (Genant et al., 1999).
Within yoga spaces, teachers and students are often exposed to conflicting claims. It is common to hear that yoga alone can prevent or even reverse osteoporosis. It is also common to hear that yoga is unsafe for anyone with osteoporosis. For yoga teachers, neither extreme position is supported by the evidence. What follows is a clearer, research-informed perspective to support safe and confident teaching.
How osteoporosis is currently diagnosed
Osteoporosis is diagnosed either by the presence of a fragility fracture or through bone mineral density assessment. Fragility fractures occur following forces that would not normally cause fracture, such as a fall from standing height resulting in a wrist or hip fracture, or a vertebral compression fracture.
Although fractures of the hip, spine, forearm, and humerus are often considered characteristic of osteoporosis, fractures at nearly all skeletal sites have been associated with the condition (Genant et al., 1999).
Prevalence data highlight how common osteoporosis becomes with age. Wright et al. (2017) reported that approximately 17 percent of men and 30 percent of women aged 50 years and older meet updated diagnostic criteria for osteoporosis. By age 80, prevalence rises to 46 percent in men and 77 percent in women. Kanis et al. (2000) estimated a lifetime risk of major osteoporotic fracture of 46 percent for women and 22 percent for men.
Osteoporosis may be primary, with no identifiable cause, or secondary to conditions such as long-term corticosteroid use, excessive alcohol intake, low calcium intake, vitamin D deficiency, smoking, antiepileptic medication use, thyrotoxicosis, primary hyperparathyroidism, chronic liver or kidney disease, rheumatoid arthritis, and diabetes.
Exercise guidelines for people with osteoporosis
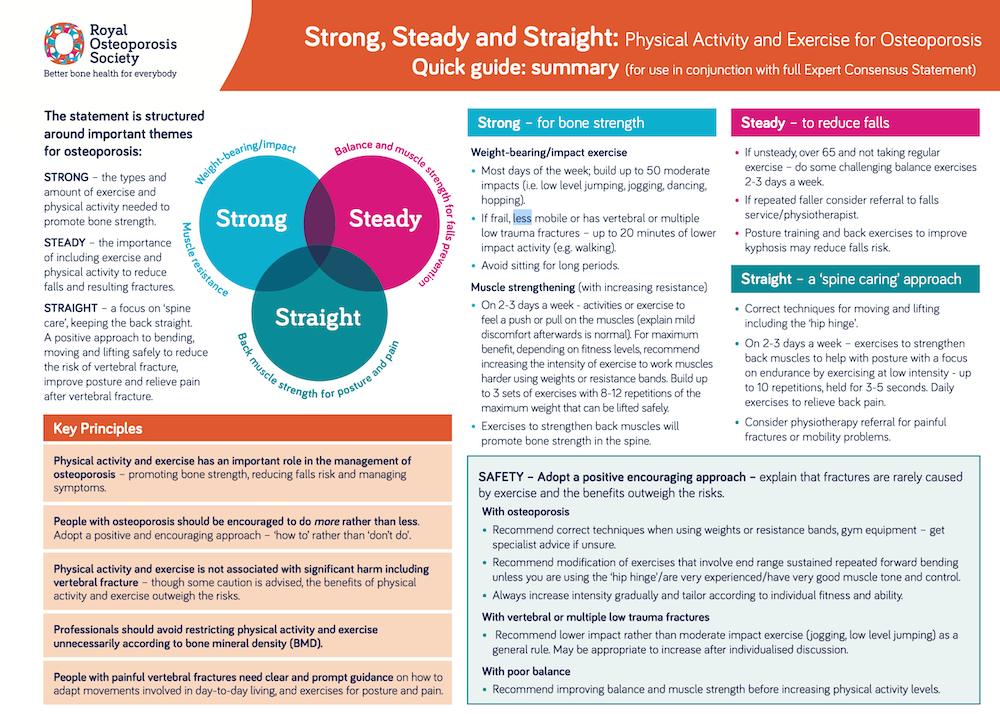
Clear guidance exists regarding exercise and osteoporosis. A UK consensus statement by Brooke-Wavell et al. (2022) recommends that people with osteoporosis should undertake:
Resistance and impact exercise to maximise bone strength
Strength and balance activities to reduce fall risk
Spinal extension exercises to improve posture and potentially reduce vertebral fracture risk
For safety, the authors recommend avoiding postures involving a high degree of spinal flexion during exercise and daily life. Individuals at higher fall risk should begin with targeted balance and strength training. People with vertebral fracture symptoms may benefit from exercise to reduce pain and improve mobility, ideally with specialist guidance to support a return to normal activities. Importantly, the authors concluded that there is little evidence of significant harm from physical activity, and that benefits generally outweigh risks.
The International Osteoporosis Foundation provides similar guidance. Aerobic activity and progressive resistance training are considered safe when intensity is initially light to moderate and increased gradually based on capacity (International Osteoporosis Foundation, n.d.). Trunk extension and abdominal stabilisation exercises are supported. Powerful twisting movements are discouraged, which can be interpreted as prioritising active, muscularly controlled movement over externally forced flexibility. Deep spinal flexion, particularly under load, should be avoided, while unloaded flexion may be appropriate for some individuals. Programmes should be supervised by qualified professionals and include muscle strengthening, balance, and coordination training.
The Royal Osteoporosis Society also encourages a positive, reassuring approach. Teachers are advised to explain that fractures are rarely caused by exercise, and that benefits outweigh risks. Extreme or loaded flexion should be modified unless individuals are well conditioned and demonstrate strong muscular control (Royal Osteoporosis Society, 2019).
Spinal rotation and side bending
Very little empirical evidence exists regarding the effects of spinal rotation and lateral flexion in people with osteoporosis (Smith and Boser, 2013). From a research perspective, there is no strong basis for advising universal avoidance of spinal rotation or side bending.
Bone is anisotropic, meaning its strength varies depending on the direction of loading. To optimise bone strength, bones must be loaded dynamically along multiple axes. Eliminating all spinal rotation may reduce stimulus along the transverse axis, potentially leaving the spine less conditioned for rotational demands encountered in daily life. As with other tissues, the spine and intervertebral discs appear to benefit most from moderate, progressive, weight-bearing movement that is well controlled.
What role can yoga play?
Yoga can play a valuable role in osteoporosis management, particularly through improving balance, coordination, body awareness, and confidence with movement. These factors are central to fall prevention, which is a major determinant of fracture risk.
However, yoga alone is unlikely to provide sufficient stimulus to maintain or increase bone mineral density over time. Lu et al. (2016) examined whether a short daily yoga practice could reverse osteoporotic bone loss. Despite the striking title of the paper, the study has been widely criticised for methodological limitations, incomplete data, and inconclusive findings.
For individuals who are largely inactive, bodyweight practices such as yoga can be an important first step in progressive loading. Over time, however, bones require greater mechanical stimulus than most general yoga classes provide. Progressive resistance training and impact loading remain the most strongly supported interventions for bone health.
For yoga teachers, the key message is integration rather than exclusion. Yoga can complement, but not replace, targeted bone-loading exercise.
References:
Brooke-Wavell, K., Skelton, D., Barker, K., et al. (2022). Strong, steady and straight: UK consensus statement on physical activity and exercise for osteoporosis. British Journal of Sports Medicine, 56, 837–846.
Genant, H., Cooper, C., Poor, G., Reid, I., Ehrlich, G., Kanis, J., Nordin, B., et al. (1999). Interim report and recommendations of the World Health Organization Task Force for Osteoporosis. Osteoporosis International, 10(4), 259–264.
Kanis, J., Johnell, O., Oden, A., et al. (2000). Long-term risk of osteoporotic fracture in Malmö. Osteoporosis International, 11(8), 669–674.
Lu, Y., Rosner, B., Chang, G., and Fishman, L. (2016). Twelve-minute daily yoga regimen reverses osteoporotic bone loss. Topics in Geriatric Rehabilitation, 32(2), 81–87.
Smith, E., and Boser, A. (2013). Yoga, vertebral fractures, and osteoporosis: Research and recommendations. International Journal of Yoga Therapy, 23(1), 17–23.
US Department of Health and Human Services. (2004). Bone Health and Osteoporosis: A Report of the Surgeon General. Rockville, MD: US Department of Health and Human Services.
Wright, N., Saag, K., Dawson-Hughes, B., Khosla, S., and Siris, E. (2017). The impact of the new National Bone Health Alliance diagnostic criteria on the prevalence of osteoporosis in the USA. Osteoporosis International, 28(4), 1225–1232.
International Osteoporosis Foundation. Exercise for individuals with osteoporosis.
https://www.osteoporosis.foundation/health-professionals/prevention/exercise/exercise-individuals-with-osteoporosis
Royal Osteoporosis Society. (2019). Strong, steady and straight: Quick guide.
https://theros.org.uk/media/0o5h1l53/ros-strong-steady-straight-quick-guide-february-2019.pdf