Low back pain is currently the leading cause of disability worldwide (Hartvigsen et al. 2018). For yoga teachers, this matters not only because many of our students experience back pain, but because the way we talk about it can meaningfully influence outcomes. One of the most powerful tools we have is not a pose, a stretch, or a cue about alignment, but the language and expectations we help create in the room.
An excerpt adapted from my book The Physiology of Yoga.
1. Most people will experience low back pain
An estimated 60 to 80 percent of people will experience low back pain at some point in their lives. This includes yoga practitioners, yoga teachers, athletes, and people who do not exercise at all. Back pain is not a sign that someone has done something wrong, moved incorrectly, or failed to protect themselves.
In around 85 percent of cases, low back pain cannot be attributed to a specific structural issue such as a disc injury, fracture, or serious pathology (Airaksinen et al. 2006). This is often referred to as non-specific low back pain. For teachers, this is an important reframe. Pain does not automatically equal damage, and the absence of a clear cause does not mean something has been missed.

2. Back pain is rarely caused by something “serious”
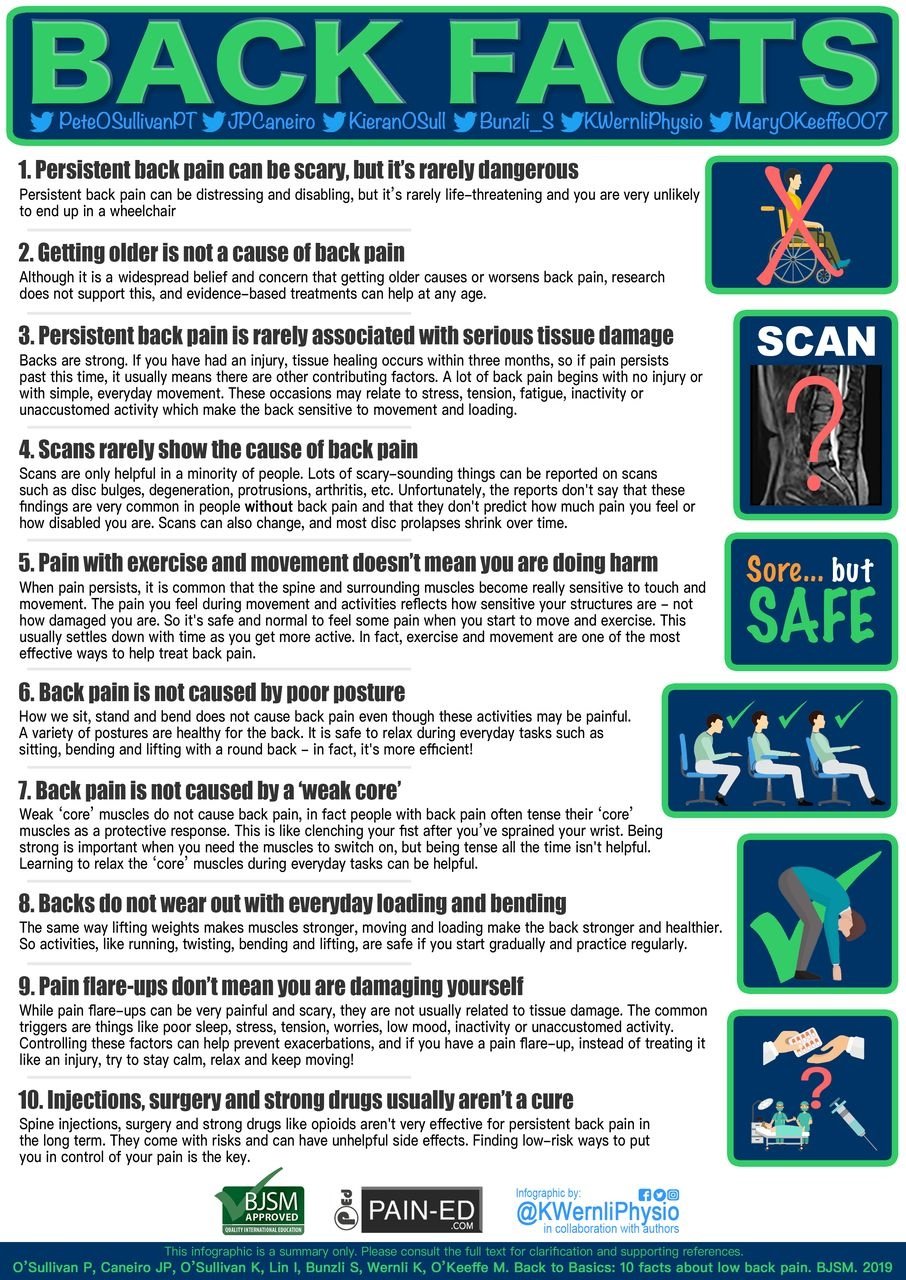
Once red flags and serious pathology are excluded, evidence consistently shows that low back pain is not a life-threatening medical condition. It does not inevitably worsen with age, and most episodes improve with time (O’Sullivan et al. 2020).
This runs counter to many messages students absorb from media, scans, and well-meaning professionals. As yoga teachers, we are often in a position of trust. Communicating calm reassurance, rather than concern or alarm, can help reduce fear and support recovery.
3. Beliefs about back pain strongly influence outcomes
Unhelpful beliefs about back pain are common, not just among the general public, but also among yoga teachers and health professionals. These beliefs include ideas such as the spine being fragile, certain movements being dangerous, or pain meaning harm.
Research shows that unhelpful beliefs are associated with higher pain levels, greater disability, increased work absenteeism, higher medication use, and greater health care seeking (Main, Foster, and Buchbinder 2010). In contrast, people who feel confident moving and believe their back is strong tend to recover better.
4. Language can increase pain through the nocebo effect
The placebo effect is widely known, where positive expectations can reduce pain or improve symptoms. The nocebo effect is the opposite. Negative expectations can increase pain or other symptoms, even when no harm is occurring (Benedetti et al. 2007).
A large review found that 49 percent of participants taking placebo pills in clinical trials reported adverse effects such as headache, nausea, or pain (Howick et al. 2018). These effects occurred even when the substance itself was inert, and sometimes even when participants were not warned about side effects. Expectation alone can drive real physiological responses.

5. Yoga cues can unintentionally trigger nocebo responses
Verbal suggestions do not need to be dramatic to have an effect. Simple, familiar cues can increase threat and fear around the back.
Examples include:
“Engage your core to protect your back.”
“Your sacroiliac joints are very vulnerable.”
“Be careful not to compress your lower back.”
While these cues are usually well-intentioned, they imply that the spine is fragile and easily damaged. Research shows that negative verbal suggestions can increase pain by triggering anticipatory anxiety and sensitising the nervous system (Benedetti et al. 2007). Over time, this can lead students to avoid movement they perceive as dangerous.
6. The human body is adaptable, not fragile
Modern physiology shows that the human body adapts to the loads placed upon it. While injury and disease are possible, the spine is designed to move, bear load, and respond positively to gradual challenge.
The concept of antifragility describes systems that become stronger when exposed to appropriate stress, rather than weaker (Taleb 2012). This does not mean pushing through pain or ignoring symptoms. It means recognising that movement and loading, when progressed thoughtfully, support tissue health rather than threaten it.
7. Movement is one of the best treatments for back pain
High-quality evidence consistently supports movement and graduated exercise for low back pain. Moving in different directions, building strength, and staying physically active are safe and beneficial for spinal health (O’Sullivan et al. 2020).
Fear-based avoidance of movement is more strongly linked to persistent pain than structural findings on scans. As teachers, encouraging students to explore movement with curiosity and confidence can be far more helpful than encouraging restriction or excessive caution.

8. Positive messaging improves pain outcomes
A positive, reassuring mindset around back pain is associated with lower pain levels, reduced disability, and less health care seeking (Beales et al. 2015). Importantly, most people are unfamiliar with the nocebo effect, yet learning about it can reduce its negative impact (Planès, Villier, and Mallaret 2016).
Around 90 percent of low back pain episodes are self-limiting and resolve within six weeks (Waddell 1987). While flare-ups can be frustrating, they are often linked to changes in activity, stress, sleep, or mood, rather than injury or structural damage.
As yoga teachers, being mindful of our language allows us to support resilience rather than fear. One of the most effective interventions we already offer is regular, varied movement. How we frame that movement may matter just as much as the movement itself.
References:
Airaksinen, O., J. Brox, C. Cedraschi, J. Hildebrandt, J. Klaber-Moffett, F. Kovacs, et al. 2006. “Chapter 4. European Guidelines for the Management of Chronic Nonspecific Low Back Pain.” European Spine Journal 15 (Suppl. 2): S192-S300.
Beales, D., A. Smith, and P. O’Sullivan, et al. 2015. “Back Pain Beliefs Are Related to the Impact of Low Back Pain in Baby Boomers in the Busselton Healthy Aging Study.” Physical Therapy 95:180-189.
Benedetti, F., M. Lanotte, L. Lopiano, and L. Colloca. 2007. “When Words Are Painful: Unraveling the Mechanisms of the Nocebo Effect.” Neuroscience 147 (2): 260-271.
Hartvigsen, J., M.J. Hancock, A. Kongsted, Q. Louw, M.L. Ferreira, S. Genevay, D. Hoy, J. Karppinen, G. Pransky, J. Sieper, R.J. Smeets, and M. Underwood. 2018. Lancet Low Back Pain Series Working Group. “What Low Back Pain Is and Why We Need to Pay Attention.” Lancet 391 (10137): 2356-2367.
Howick, J., R. Webster, N. Kirby, and K. Hood. 2018. “Rapid Overview of Systematic Reviews of Nocebo Effects Reported by Patients Taking Placebos in Clinical Trials.” Trials 19 (1): 674.
Main, C.J., N. Foster, and R. Buchbinder. 2010. “How Important Are Back Pain Beliefs and Expectations for Satisfactory Recovery From Back Pain?” Best Practice & Research Clinical Rheumatology 24 (2): 205-217.
O’Sullivan, P.B., J.P. Caneiro, K. O’Sullivan, I. Lin, S. Bunzli, K. Wernli, and M. O’Keeffe. 2020. Back to Basics: 10 Facts Every Person Should Know about Back Pain. British Journal of Sports Medicine 54 (12): 698-699. https://doi.org/10.1136/bjsports-2019-101611.
Planès, S., C. Villier, and M. Mallaret. 2016. “The Nocebo Effect of Drugs.” Pharmaceutical Research and Perspectives 4 (2): e00208. https://doi.org/10.1002/prp2.208.
Taleb, N.N. 2012. Antifragile: Things That Gain From Disorder. Vol. 3. Random House Incorporated.
Waddell, G. 1987. “1987 Volvo Award in Clinical Sciences. A New Clinical Model for the Treatment of Low-Back Pain.” Spine 12 (7): 632-644.