Rheumatoid arthritis, often shortened to RA, is one of the most common inflammatory conditions yoga teachers encounter. Yet it is also one of the most misunderstood.
Rather than diving into complex immunology, this week’s newsletter takes a practical teaching lens. Here are eight things every yoga teacher should know when working with students who have rheumatoid arthritis.
1. Rheumatoid arthritis is not a wear and tear condition
RA is a systemic autoimmune disease. That means the immune system mistakenly attacks healthy tissue, particularly the lining of joints.
This is very different from osteoarthritis. In RA, pain, stiffness, and swelling are driven by inflammation, not by joints being worn out or weak.
Teaching takeaway:
Stretching alone is not the solution. Strength, control, pacing, and recovery matter far more than increasing range of motion.

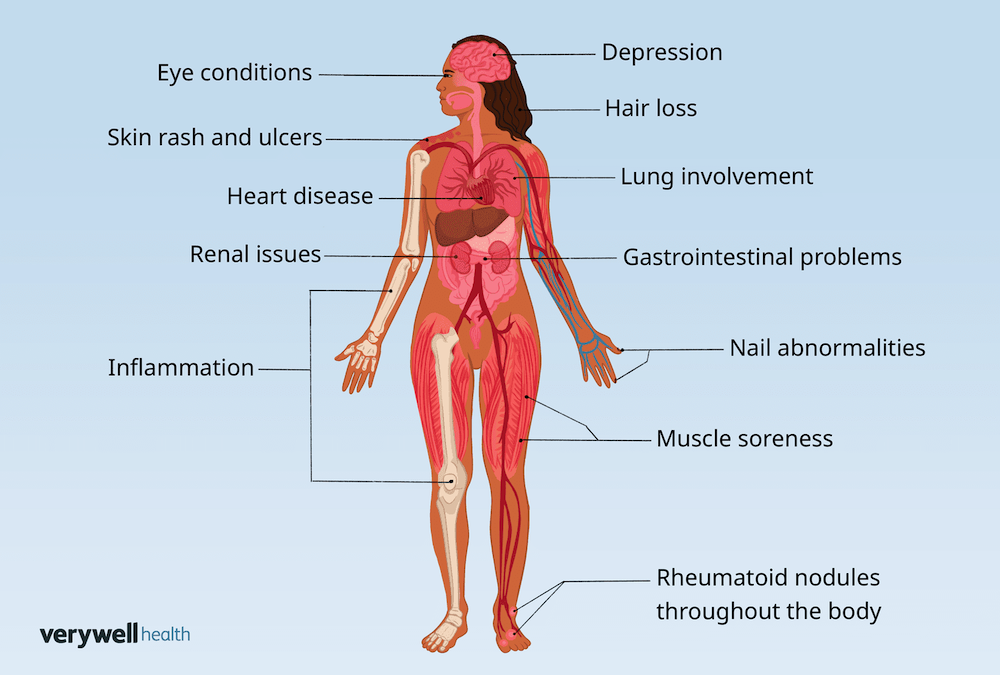
2. RA affects the whole body, not just the joints
Although RA commonly affects the hands and feet, it is a whole-body condition. Chronic inflammation is associated with fatigue, muscle loss, reduced bone density, and increased cardiovascular risk (Metsios et al 2008; Radner et al 2017).
For many students, fatigue is the most limiting symptom, sometimes more than pain.
Teaching takeaway:
Energy management is as important as joint care. A shorter, well-paced practice may be far more beneficial than a long class.
3. Symptoms fluctuate from day to day
RA symptoms are not consistent. A student may feel relatively strong one week and significantly limited the next, even when medication is stable.
Morning stiffness is common and may last longer than 30 to 60 minutes. Flares can occur without a clear trigger.
Teaching takeaway:
Avoid assumptions. Always offer options and frame practice as responsive rather than progressive.
4. RA often affects joints symmetrically
RA commonly presents on both sides of the body, especially in the hands and feet. Swelling, warmth, and tenderness may be visible.
Symmetry in disease does not mean symmetry in capacity. One wrist or shoulder may still tolerate load better than the other.
Teaching takeaway:
Avoid rigid ideas of bilateral balance. Encourage students to work with what they feel rather than what a shape looks like.
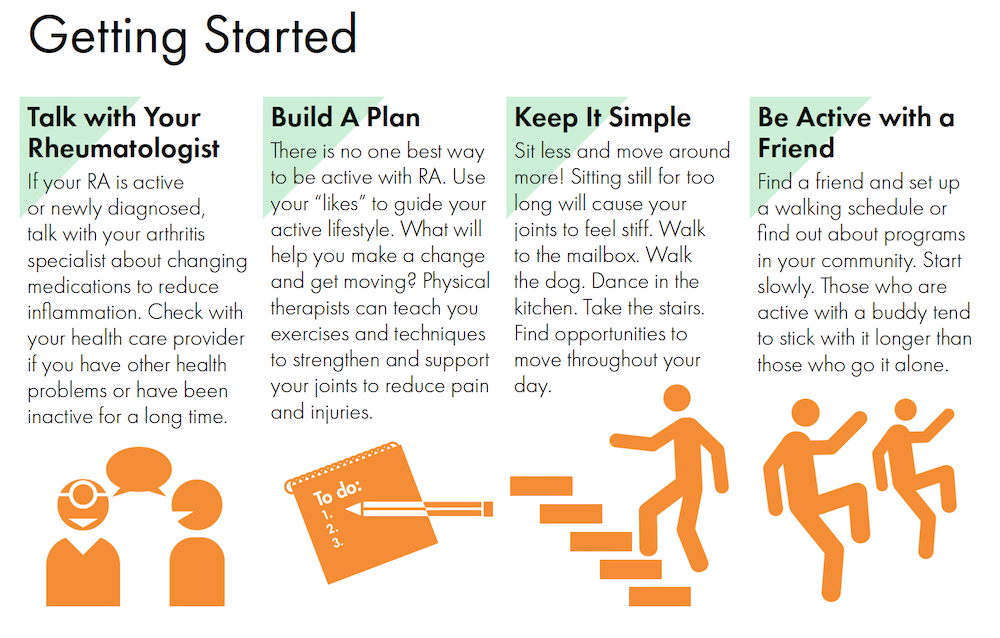
5. Exercise is safe and beneficial for people with RA
A large overview of systematic reviews found that aerobic exercise, strength training, and hand exercises all improve function and reduce fatigue in people with RA (Hu et al 2021).
Importantly, any exercise is better than no exercise. Fear of movement is a major barrier, even among healthcare professionals (Munneke et al 2004).
Teaching takeaway:
Reassurance matters. Help students understand that appropriately dosed movement supports joint health rather than damaging it.
This great infographic was produced by the American college of Sports Medicine:
6. Yoga can help, but it is not a treatment
A systematic review and meta-analysis found that yoga may improve physical function, grip strength, and overall disease activity in people with RA (Ye et al 2020).
However, yoga did not significantly reduce pain, joint swelling, or inflammatory markers. Yoga supports wellbeing, but it does not replace medical treatment.
Teaching takeaway:
Position yoga as supportive, not curative. This builds trust and protects students from unrealistic expectations.

7. Joint protection matters more than flexibility
Inflamed joints do not respond well to long static holds or aggressive end range stretching, especially during flares.
Strength, proprioception, and controlled movement help distribute load away from irritated joint surfaces.
Teaching takeaway:
Prioritise steady transitions, shorter holds, props, and active engagement over depth.

8. Individualisation is the most important skill
There is no single “RA friendly” sequence. Disease stage, medication, fatigue, pain levels, and confidence all influence what a student can do on a given day.
Your role is not to fix RA, but to support safe participation, autonomy, and confidence in movement.
Teaching takeaway:
Ask questions, offer choices, and normalise rest. Good teaching is responsive, not prescriptive.
References:
Hu, Z., Yang, B., Tang, L., Wang, Y., and Lin, J. (2021). The effect of physical exercise on rheumatoid arthritis: An overview of systematic reviews and meta analyses. Frontiers in Physiology, 12, 771322.
Lin, Y. J., Anzaghe, M., and Schülke, S. (2020). Update on the pathomechanism, diagnosis, and treatment options for rheumatoid arthritis. Cells, 9(4), 880.
Metsios, G. S., Stavropoulos Kalinglou, A., Panoulas, V. F., Wilson, M., and Kitas, G. D. (2008). Cardiovascular risk management in rheumatoid arthritis. Rheumatology, 47(4), 434–439.
Munneke, M., de Jong, Z., Zwinderman, A. H., et al. (2004). The effects of exercise on disease activity and functional ability in rheumatoid arthritis. Arthritis and Rheumatism, 51(6), 909–915.
Radner, H., Yoshida, K., Hmamouchi, I., et al. (2017). Treatment patterns of multimorbidity in rheumatoid arthritis. Rheumatology, 56(4), 594–604.
Romão, V. C., and Fonseca, J. E. (2021). Etiology and risk factors for rheumatoid arthritis: A state of the art review. Frontiers in Medicine, 8, 689698.
Ye, X., Chen, Z., Shen, Z., Chen, G., and Xu, X. (2020). Yoga for treating rheumatoid arthritis: A systematic review and meta analysis. Frontiers in Medicine, 7, 586665.